
Scope of Problem
Healthcare environments bring together vulnerable patients, high-risk exposures, and ethical obligations. While vaccination has long been foundational to infection prevention, post-COVID data reveal declining booster uptake and persistent hesitancy among segments of the healthcare workforce (Giubilini et al., 2023).
For students and faculty, vaccination policy is no longer theoretical; it shapes clinical placement requirements, employment eligibility, and professional ethics. Understanding why healthcare workers (HCWs) resist or accept mandates is essential for preparing graduates who can lead, comply, and communicate effectively in real-world healthcare settings.
Research Overview: Key Findings
Research on HCWs responses to mandatory vaccination policies indicates that vaccination behavior is shaped less by enforcement alone and more by how policies align with workforce perceptions, trust, and professional identity (Giubilini et al., 2023). While mandates can increase short-term uptake, sustained acceptance depends on how effectively institutions address the factors influencing hesitancy and compliance.
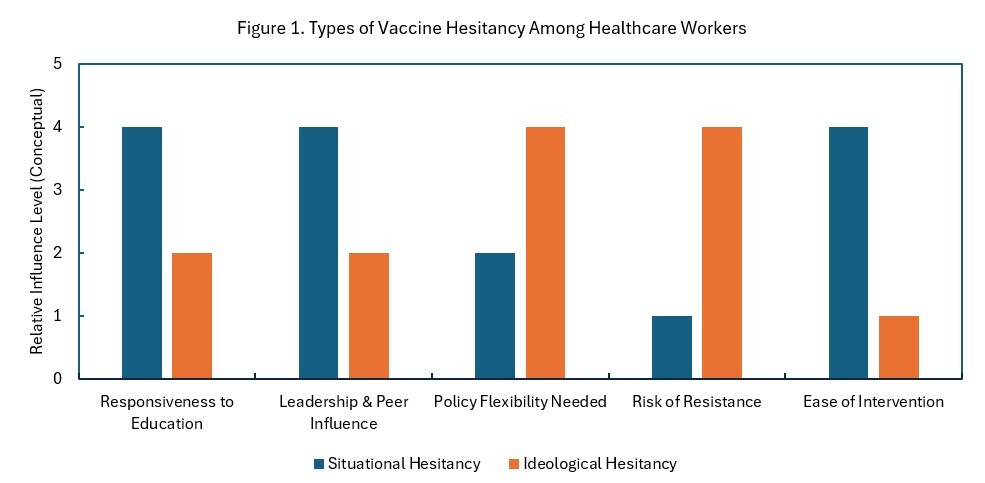
Evidence shows that vaccine hesitancy among HCWs reflects two primary patterns: Situational or Ideological Hesitancy. Situational hesitancy is commonly associated with low perceived personal risk, vaccine fatigue, time constraints, and emotional burnout (Wang et al., 2024). This form of hesitancy often results in delayed or passive noncompliance and is typically responsive to targeted education, leadership and peer engagement, and practical support that facilitates vaccination. In contrast, ideological hesitancy is more closely linked to deeply held cultural, religious, or political beliefs and is less responsive to education alone. Addressing ideological hesitancy requires trust-building, culturally competent communication, and flexible options to facilitate vaccination (Okpani et al., 2024).
Across both patterns, research consistently identifies motivators that increase vaccine uptake. Framing vaccination as a professional duty of care, emphasizing protection of patients and family members, and reinforcing vaccination as a patient safety standard strengthens acceptance (Centers for Disease Control and Prevention [CDC], 2024). Clear institutional policies, visible leadership participation, and peer modeling further normalize vaccination as a professional expectation (Wang et al., 2024).
Together, these findings underscore the importance of tailoring vaccination policies to the type of hesitancy encountered. Figure 1 presents a conceptual comparison of situational and ideological hesitancy, highlighting differences in responsiveness to education, leadership influence, policy flexibility needs, and intervention complexity. Policies that account for these distinctions are more likely to achieve sustained compliance than enforcement-only approaches.

Policy Options and Alternatives
Healthcare institutions have employed a range of approaches to increase vaccination uptake among healthcare workers, each with distinct advantages and limitations. The effectiveness of these approaches depends on workforce composition, institutional culture, and the types of hesitancy present.
Option 1: Enforcement-Only Mandates
This approach requires vaccination as a condition of employment and may include disciplinary consequences. Enforcement-only mandates can rapidly increase coverage, particularly during public health emergencies. For example, a five-year study at Virginia Mason Medical Center with approximately 5,000 employees reported vaccination rates exceeding 97% in the first year and remaining above 98% thereafter, with minimal workforce attrition (Rakita et al., 2010). However, when implemented without adequate communication or support, such mandates may erode trust, provoke resistance, and create ethical challenges, thus limiting effectiveness in settings marked by ideological hesitancy or institutional mistrust (Giubilini et al., 2023).
Option 2: Voluntary Education and Incentive-Based Programs
Voluntary strategies emphasize education, risk communication, and incentives such as paid time off or recognition. These approaches support autonomy and foster trust, particularly among healthcare workers experiencing situational hesitancy. However, uptake is typically slower, and voluntary programs may be insufficient when rapid or widespread coverage is required (Wang et al., 2024).
Option 3: Integrated Mandate and Engagement Approach
An integrated approach combines clear vaccination requirements with targeted education, leadership engagement, and accessible vaccination options. By reducing practical barriers while reinforcing professional and ethical expectations, this model addresses both situational and ideological hesitancy (Shen et al., 2020).
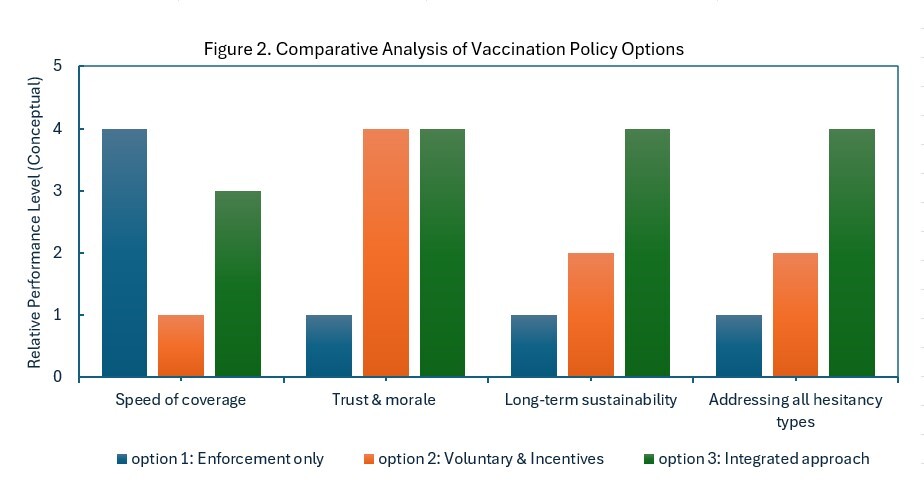
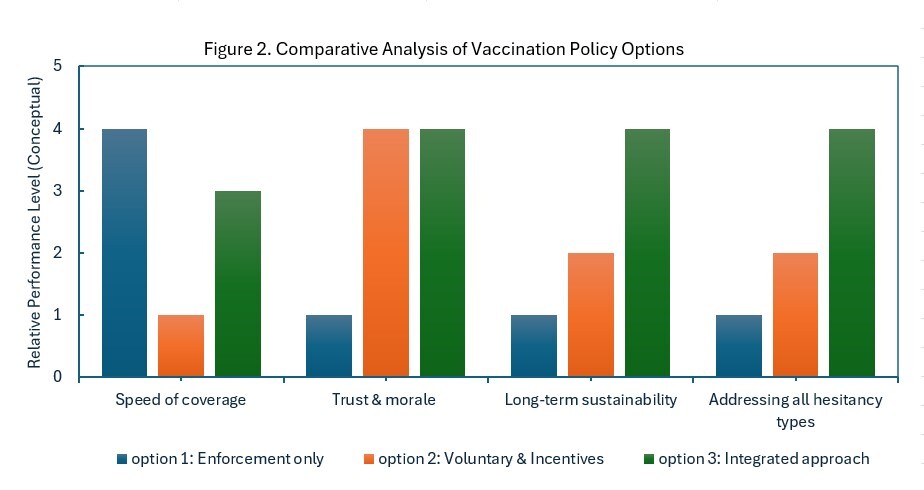
However, no single strategy is universally effective. Selecting an appropriate approach requires assessing local workforce hesitancy patterns while balancing public health objectives with organizational trust and engagement. Figure 2 illustrates how integrated vaccination strategies that combine mandates with education, leadership engagement, and accessible implementation address both situational and ideological hesitancy more effectively than enforcement-only or voluntary approaches. This conceptual model supports more sustainable uptake by reducing barriers while reinforcing professional norms and institutional trust.
Recommendations
Healthcare institutions and academic programs should adopt vaccination strategies that reflect varied forms of workforce hesitancy. Evidence indicates that integrated approaches combining clear policy expectations with education, leadership engagement, and logistical support achieve more sustained uptake than enforcement alone (Okpani et al., 2024).
Substantiation from large hospital settings shows that mandates reinforced by active engagement strategies such as education and reminder systems can increase healthcare worker vaccination coverage from approximately 23% to nearly 78%, with engagement efforts converting a substantial proportion of previously noncompliant staff (Di Lorenzo et al., 2021). Consistent with these findings, integrated strategies are associated with more sustainable uptake and fewer workforce disruptions than enforcement-only approaches (Okpani et al., 2024). Additionally, vaccination policies should be transparent, consistently communicated, and grounded in patient safety standards, with clearly defined and accessible exemption and compliance processes to reinforce professional alignment (CDC, 2024).
Institutions should prioritize targeted education and communication to address situational hesitancy. Educational efforts should emphasize relevance over volume, focusing on risk, benefits, and real-world implications for patients, families, and healthcare teams. Messaging is most effective when delivered through trusted channels and reinforced by peer and leadership role models (World Health Organization [WHO], n.d.).
Finally, visible leadership engagement should be treated as a core vaccination strategy. When leaders and supervisors model compliance and engage in open dialogue, vaccination is normalized as a professional expectation rather than perceived as an imposed requirement. Leadership visibility further supports trust-building, particularly in environments affected by skepticism or fatigue (Okpani et al., 2024). Figure 3 illustrates how the recommended strategies can be operationalized within healthcare and academic settings.

Conclusion
Healthcare worker vaccination policies remain central to patient safety and workforce protection. Evidence indicates that effectiveness depends not solely on enforcement, but on alignment with workforce perceptions, professional values, and institutional trust. Distinguishing between situational and ideological forms of vaccine hesitancy provides a clearer framework for understanding responses to vaccination mandates. As summarized in Figure 1, different forms of hesitancy require distinct engagement strategies, highlighting the limitations of uniform, one-size-fits-all policy approaches.
Importantly, because the studies reviewed differed in design, data sources, and levels of analysis, it was not appropriate to combine their results into a single quantitative estimate. However, the narrative synthesis consistently shows that vaccination mandates are most effective when embedded within integrated strategies that combine clear policy expectations with education, leadership visibility, and ongoing evaluation. For academic programs and healthcare organizations, this integrated approach advances long-term public health goals while allowing policies to adapt to evolving workforce needs.